Classifying movement patterns in back pain – that's what specialist physiotherapists have done for years. Through observation, testing, assessment. It takes time, costs money, and two specialists don't always reach the same conclusion. The BackTracker study (Liu et al., 2026) now shows: a neural network, trained on one expert's classifications, does the same job from a simple video – in seconds, with 92% accuracy.
Spotting back pain type from video – what specialists used to do, AI now does in seconds
At a glance
AI analyses a video of your backward bend and identifies with 92% accuracy whether you have a flexion or extension problem. That determines which exercises will help you. The underlying tech (camera + neural network) exists as open source – in theory a weekend project with Python and MediaPipe.
Stay on top of AI training & analysis? One click — and Google shows you my articles first.
Add as a preferred source on GoogleWhat is this actually about?
Non-specific low back pain (NSLBP) – back pain without a clear disc herniation or fracture – affects almost everyone at some point. The problem: "non-specific" doesn't mean "all the same." Different movement patterns lie behind the pain, and depending on the pattern you need completely different exercises.
Simplified, there are two main types. With the flexion pattern (FP), your lumbar spine bends forward too much – typical for people who sit a lot and bend almost entirely from the back rather than the hips. Here, exercises that improve hip flexion and stabilise the lumbar spine tend to help – things like hip hinges or controlled deadlift variations. With the extension pattern (EP) it's the opposite: your lumbar spine over-extends when standing or bending backwards. That calls more for core stabilisation and posterior pelvic tilt – dead bugs, planks, pelvic tilts. (Important: these are tendencies, not therapy recommendations. Which exercises suit you depends on more than just the movement pattern.) It sounds simple, but that's exactly where the risk lies: someone with a flexion problem doing extension exercises can get worse instead of better. The type decides the therapy – and the exercises you'd better leave out.
This classification has existed for years – just done manually, by trained specialists. BackTracker automates exactly this step.
How it works: camera, silhouette, AI
The procedure is surprisingly simple. 90 people with back pain were filmed from the side as they bent forwards and backwards – perfectly ordinary movements, no acrobatic tests. From the videos, the software automatically extracted black-and-white silhouettes of the back: 80 images per person at various bending angles. So the AI doesn't see your face, doesn't see your clothing – only the contour of your back in motion.
These silhouettes fed a neural network that learned to distinguish FP from EP. The learning works like any supervised learning approach: an experienced physiotherapist had manually classified all participants beforehand, and the AI takes over this pattern recognition. It picks out the relevant features itself – curvature, angle trajectories, coordination between hip and lumbar spine.
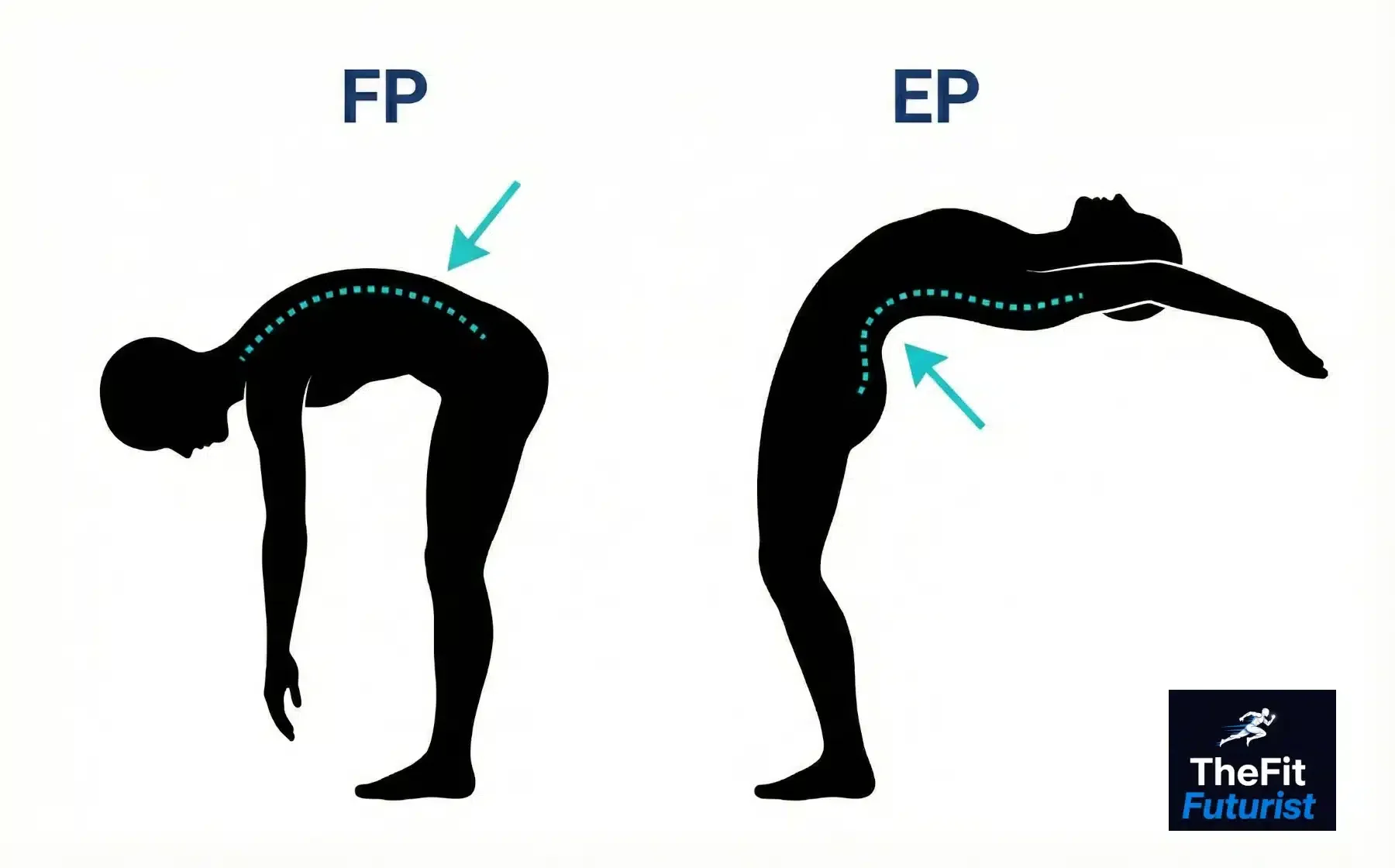
This is how the AI sees the back: black-and-white silhouettes during the backward bend. On the left a flexion pattern (FP), on the right an extension pattern (EP). The differences in lumbar spine curvature are what the neural network classifies.
WHAT IS POSE ESTIMATION?
Pose estimation is a computer vision technique that automatically detects body landmarks – shoulder, hip, knee, ankle and so on – from a normal camera image. Google's MediaPipe does this for free in real time, even on a phone. The same tech powers fitness apps that check your squat form.
The results: 92% – and questionnaires don't help
The model identifies the correct back pain type from a video of the backward bend in 92% of cases. For comparison: the literature shows lower typical agreement when two different specialists independently assess the same person. In concrete terms: the AI reproduces the expert's assessment more consistently than two specialists typically agree with each other.
What was analysed? | Accuracy | Assessment |
|---|---|---|
Backward bend video only | 92% | Best result |
Forward bend video only | 87% | Good, but weaker |
Both videos combined | 86% | Surprising: more data doesn't help |
Pain questionnaires only | 64% | Barely better than a coin flip |
Video + questionnaires combined | 72% | Questionnaires make the result worse |
Classification accuracy by data source – data: Liu et al. (2026)
The most interesting point in the table: self-assessment questionnaires – "How bad is your pain?", "What can't you do any more?" – actually worsen the classification when added to the video data. Your self-perception and your actual movement pattern clearly don't match up well. The camera sees what you don't feel.
And why does the backward bend beat the forward bend? Because in backward bending, the lumbar spine shows particularly clearly whether it's working too much or too little. In forward bending, hip flexibility and hamstring tension muddy the picture – more noise, less clear signal.
What does this mean for you?
Imagine the following scenario: you have back pain, you put your phone on a shelf, film yourself doing a backward bend, and an app tells you: "Extension pattern – here are three exercises that target it specifically. And please skip these two." The whole thing costs nothing and takes minutes. That's the goal of this research.
We're not quite there yet. BackTracker is a study, not an app in the store. But the tech behind it isn't rocket science. Pose estimation via phone camera has been around for ages – every other fitness app uses it to rate your squat form. The jump from "counts your squats" to "identifies your back pain pattern" is conceptually smaller than you might think.
In practice, for a usable recording you need: a side-on camera position, fitted clothing (no loose shirt that hides the back's contour), and enough distance so your whole body is in frame. Topless isn't necessary – a sports shirt is fine, as long as the AI can cleanly pick up your spinal contour.
The honest assessment
92% accuracy sounds good – and it is. But there are a few things you should know before reading too much into it.
The study had 90 participants. For a feasibility proof that's solid; for a finished product it would be too few. On top of that, a single physiotherapist classified all participants. That's methodologically clean – no conflicting judgements – but it also means: the AI learns one person's assessment, not a universal truth. Whether other experts would have judged all participants identically remains open.
And the most important point: the study proves that the classification works – not that the exercises derived from it actually help faster than standard therapy. "We can identify the type" isn't the same as "we know type-specific exercises work better." That second step still has to come.
NOT A REPLACEMENT FOR A DOCTOR
BackTracker classifies movement patterns – it doesn't diagnose causes. The system doesn't detect disc herniations, stenoses or inflammation. If you have severe, persistent or radiating pain, see a doctor, not an app. AI tools like this are supplements, not substitute diagnoses.
The DIY angle: could you build this yourself?
Short answer: yes, the technical building blocks are open source and freely available. Google's MediaPipe detects body landmarks from any phone video in real time. OpenCV processes the video frames. And a small neural network in PyTorch, or even a rule-based approach with Scikit-learn, can classify angle trajectories. Claude or ChatGPT will generate the code for you in an hour.
But – and this is the decisive catch – the code isn't the problem. The problem is: how does the AI know what's "right" and what's "wrong"? It needs labelled data. Someone with expertise has to watch videos and say: "That's FP, that's EP." Without these labels, you train a system that recognises patterns but doesn't know which patterns are relevant. The prompt paradox in its purest form: no good training data without domain knowledge.
Personally, this is a project I want to try. Too much sitting, too little movement in daily life – yes, the obvious fix would be more of the latter, but until then, that's a classic precondition for a flexion pattern. A personal posture tracker that records over weeks how my lumbopelvic rhythm (the ratio of hip to lumbar flexion) shifts would be a concrete feedback tool. Not a clinically validated system, but a working prototype that shows me whether my mobility exercises actually change anything – or whether I'm just imagining it. If something comes of it, you'll read about it here.
DIY TECH STACK TO GET STARTED
Pose estimation: MediaPipe Pose (Google, free, 33 keypoints in real time). Video processing: OpenCV. Classification: Scikit-learn for rule-based angle analysis, PyTorch for your own neural network. Concrete starting point: Nick Nochnack's MediaPipe Pose tutorial on GitHub – from empty script to keypoint tracker with angle calculation in 90 minutes.
Bottom line
BackTracker delivers a convincing proof of concept: AI can identify back pain types from video recordings – fast, scalable and with a high hit rate. 90 participants, two phenotypes, no long-term comparison – the study isn't a finished product. But the direction is right, and the tools are open source. For the curious: install MediaPipe, set up your phone, film a backward bend, plot the keypoints. In an hour you'll see what the AI sees.
92% accuracy from a single video of a backward bend. No expensive motion capture, no lab – one camera and a neural network. But don't forget: the AI recognises patterns, it doesn't understand pain.
Source: Liu Z, Hicks Y, Sheeran L. BackTracker: Machine learning to identify kinematic phenotypes for personalised exercise management in non-specific low back pain. Int J Med Inform. 2026;211:106335. DOI: 10.1016/j.ijmedinf.2026.106335 | Abstract on PubMed (full text not freely available)


